


The genetic underpinnings of severe staph infections
In a large collaborative effort, an international team of researchers describes a genetic mutation that predisposes individuals to severe staphylococcus infections. The research, in collaboration with the Babraham Institute, appears in the latest edition of Science.
Staphylococcus aureus is usually harmless. Many of us host colonies of this bacterium in our noses and on our skin without suffering more than the occasional rash. But some strains of staph—particularly MRSA—can turn deadly, leading to pneumonia and sepsis that claims 20,000 lives in the U.S. each year. Now a new study describes a mutation that predisposes some individuals to severe staph infection.
Babraham Institute researcher Adrian Liston collaborated with Belgian doctors Isabelle Meyts, Rik Schrijvers, and Carine Wouters, to investigate the genetic and immunological cause of the disease.

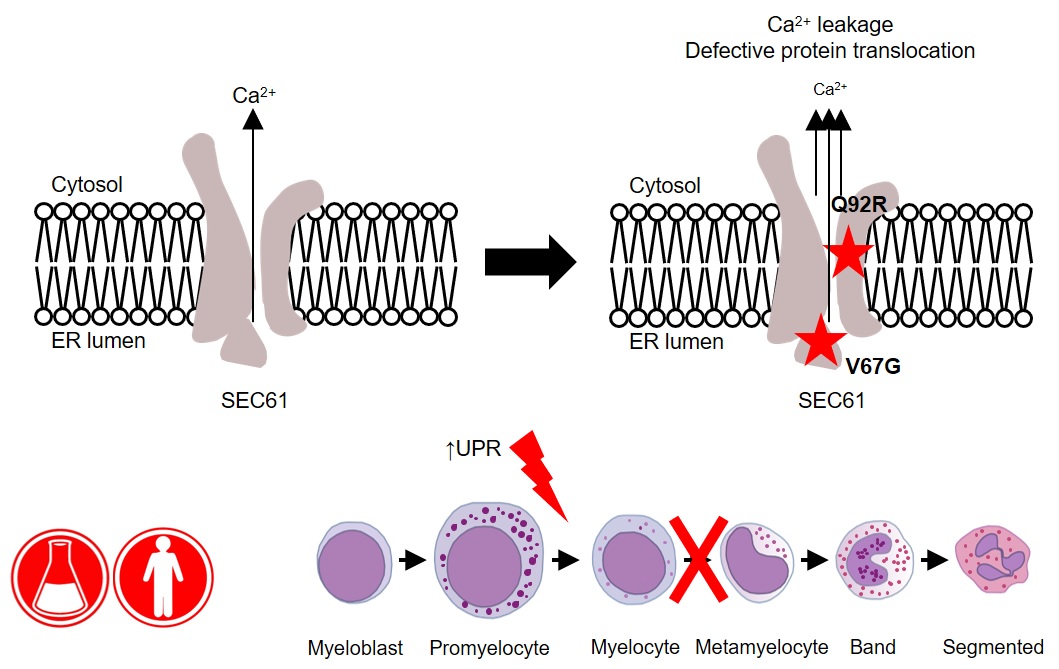
The research, published in Science, describes a mutation in the OTULIN gene in patients who suffer life-threatening staph infections. “In a collaborative effort, several unrelated patients were identified with identical severe clinical presentations and we found a common genetic cause of the disease”, says Frederik Staels, MD, and PhD student at the University of Leuven in Belgium.
"We have characterized severe Staphylococcus aureus infection at the genetic, cellular, immunological, and clinical levels," says Dr. András Spaan, a clinical microbiologist working at The Rockefeller University in New York, who was one of the coordinators of this large international effort. "By integrating these levels, we have been able to establish causality and provide clues for future pharmaceutical interventions."
The study indicated that about 30 percent of people with this OTULIN mutation develop severe disease. This risk was reduced in patients that had acquired specific anti-staph antibodies, while patients without such neutralizing antibodies remained at very high risk of developing severe infections. “This is a potential path to protecting this at-risk patients”, explains Prof Adrian Liston, “the protected patients had acquired anti-staph antibodies through natural exposure, with each exposure being a high-risk gamble for life-threatening infection. If these patients can be identified and vaccinated, the anti-staph antibodies they gain through vaccination may protect them from serious illness”.
"Studies on these disorders can act as a compass," Prof Humblet-Baron, University of Leuven, says, “They bring new mechanistic insights about the interaction between hosts and pathogens, which can also benefit the general population with better understanding about staph infection pathogenesis.”
“From a clinical point of view, this work is of great relevance to physicians confronted with patients manifesting severe, life-threatening episodes of skin and/or lung inflammation, necessitating prompt recognition and treatment,” says Prof. Wouters, pediatric rheumatologist at the University of Leuven.
Read the paper over at Science.
 Adrian Liston
Adrian Liston